What causes craniosynostosis?
Craniosynostosis is a rare birth anomaly and is present in about three to five cases per 10,000 live births. The most common type is sagittal synostosis, followed by metopic synostosis, followed by unilateral coronal craniosynostosis and lambdoid synostosis is the rarest. Associated syndromic conditions such as Apert syndrome or Crouzon syndrome are quite rare. Doctors and scientists are not sure of the exact cause of craniosynostosis. Some think it is a genetic condition, while others think the premature closure is caused by the abnormal suture itself and still others believe that it is an abnormality of the dura which is the covering overlying the brain which causes premature fusion of the suture.
When and why is treatment required?
The indications for surgical intervention include the following:
- Prevention of elevated intracranial pressure that can occur in some patients with uncorrected craniosynostosis.
- Prevention of progression of the skull deformity.
- Prevention of progression of the facial deformity.
- Optimization of growth potential of the brain.
The general consensus currently holds that the best time for surgical repair is between three and six months of age. A delay in surgery typically leads to continuation of the deformity of the craniofacial skeleton. In addition, if increased intracranial pressure is present, this will adversely affect the development of the child.
How is craniosynostosis treated?
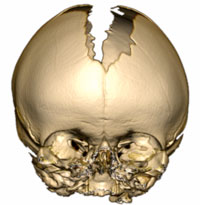
A three‑dimensional CT scan is obtained in suspected cases of craniosynostosis to confirm the diagnosis and to aid in surgical planning.
Craniosynostosis is treated with surgical correction. A team of surgeons consisting of a neurosurgeon and a craniofacial surgeon performs the surgery. The surgery can be done with an open technique or with a minimally-invasive endoscopic approach, depending on the condition and timing of repair. At Children’s Minnesota, the Neurosurgeon and Craniofacial surgeon collaborate before the procedure and then work together for the entire duration of the surgery.
The child is cared for in the pediatric intensive care unit for a few days after surgery. Most children resume a regular diet soon after the procedure and recovery quickly. It is rare but on occasion a child benefits from a secondary corrective surgical procedure at a later date. Occasionally a molding helmet is also helpful after surgical correction, but this is rarely needed. The child is then followed in the multidisciplinary Craniosynostosis Clinic to monitor growth and development.